The FDA regulates food safety, tobacco products drugs vaccines and medical devices among other things. The agency as we know it today came to be due largely to 3 health crises in the 20th century – the Diphtheria Antitoxin crisis of 1901, the Elixir Sulfanilamide crisis of 1937 and the Thalidomide crisis of 1961.
Prior to 1901, the only federal body that looked out for food and drug safety in the US was the Department of Agriculture’s (USDA) Bureau of Chemistry ran by Harvey Wiley. Wiley’s advocacy was aided by a crisis in 1901. At the beginning of the 20th century, there was no cure for diphtheria. In the US, there were about 200,000 cases per year with a death toll of about 15 000. With the introduction of the diphtheria antitoxin, attempts were made to vaccinate all children. On October 26 , 1901, a five-year-old girl died in St Louis, MO after receiving the vaccine. The cause of death was tetanus. Over the next weeks, other children died after receiving the antitoxin, which came from the St Louis City Health Department.
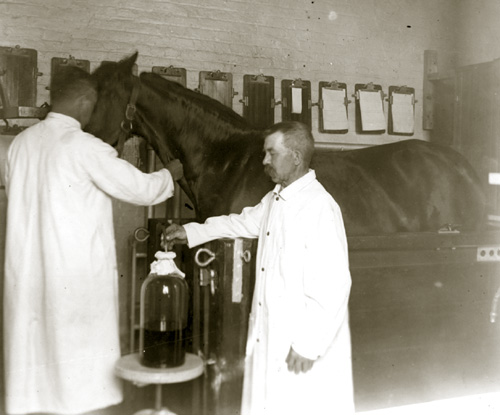
Now the antitoxin was made by injecting horses with the diphtheria bacterium and collecting the horse serum. Investigations after these deaths revealed that a horse named Jim, which had been used to produce the serum, had tetanus. It also revealed several other shortcomings at the City Health Department including mislabeled bottles, no testing of sera and continued use of the horse Jim even though the officials knew that it had contracted tetanus. In all 13 children died. Around the same time, a similar tragedy was occurring in New Jersey. Almost 100 cases of post-vaccination tetanus was recorded after administration of the small pox vaccine. In all 9 children died.
The public outrage after these events lead o the passing of the Biologics Act in 1902. In 1906, the Food and drug Act was passed.The Act prohibited, under penalty of seizure of goods, the interstate transport of food that had been “adulterated”. Wiley’s Bureau of Chemistry became the enforcer of this law. In 1927, his Bureau was renamed the Food, Drug, and Insecticide organization and shortened to the Food and Drug Administration (FDA) a few years later.

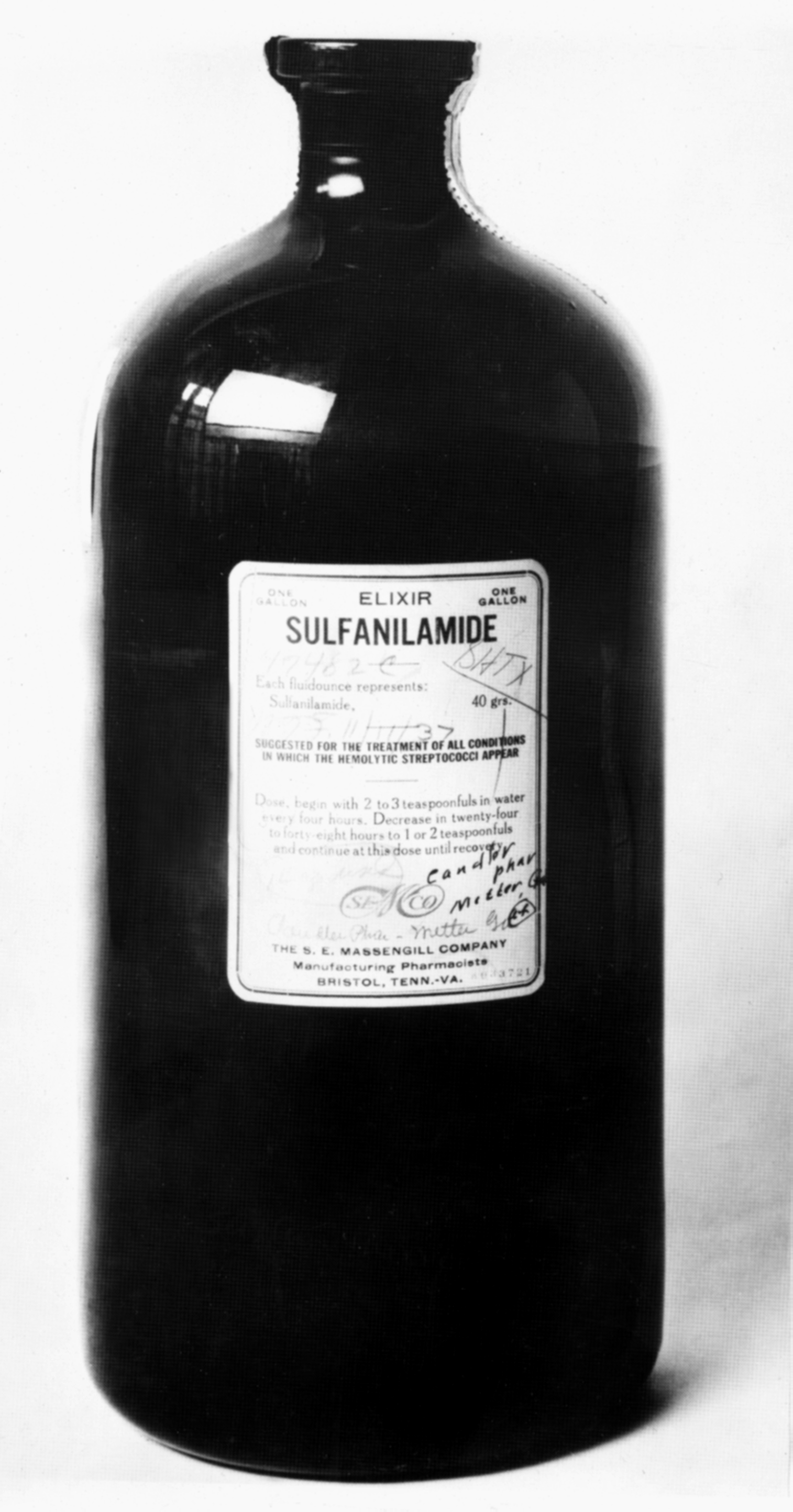
In the mid-1930s the antibiotic sulfanilamide came to the US market form Europe. It soon became the first line of treatment for streptococcal infections. It came in tablet and powder forms. Due to it’s taste, consumers, especially in the South, wanted a liquid version which would be easier to administer to children. In 1937, Harold Cole Watkins, the chief chemist at S.E. Massengill Company of Bristol, TN introduced the drug in it’s liquid form. Mr Watkins realized that sulfanilamide was soluble in diethylene glycol. The solvent that gave the mixture a sweet raspberry-like taste. He added extra raspberry flavor and coloring. Though he tested the mixture for taste, appearance and fragrance, he never bothered to test it for toxicity in humans or animals. Diethylene glycol, otherwise known as antifreeze, is rather poisonous.
In September 1937, the Massengill Co shipped 600 cases (about 268 gallons) all over the country. It was named the Elixir Sulfanilamide-Massengill.
On October 11, 1937, AMA officials in Chicago were informed of 6 deaths form a liquid sulfanilamide formulation in Tulsa, OK.There were also reports of deaths form Kansas City. On Oct 14, a NY physician tipped off the FDA about deaths from the Elixir Sulfanilamide. Meanwhile the deaths mounted. By Oct 17, it was apparent to the Masengill Co, the AMA as well as the FDA that the Sulfanilamide Elixir was causing deaths and that they had a crisis on their hands. Massengill Co, having been notified of the deaths was trying to recall the drug. The FDA urged the Massengill Company to send a follow-up telegram containing the caution “Product may be dangerous to life” to it’s salesmen.
Realizing the catastrophe at hand, the FDA dispatched all it’s 238 agents to round up all the bottles of the elixir on the market. The tales of how most of the bottles were rounded up in an era of relatively low level of mass communication can be the plot of a major Hollywood blockbuster.
Of the 268 gallons shipped, 267 gallons are confiscated. A gallon of the elixir was consumed in various parts of the country leading to 105 dead, including 34 children.
FDA and AMA had in the interim asked Dr Geiling, Head of the Department of Pharmacology at the University of Chicago to examine the elixir. Working on this project was one Frances Oldham Kersey, who almost 30 years later played a key role in the thalidomide crisis. The Geiling team analyzed the ingredients of the Elixir and found it to contain sulfanilamide, diethylene glycol, color and flavoring. They synthesized an elixir according to the same proportions and using rats, administered one of four solutions – the Massengil Elixir, their synthetic elixir, just sulfanilamide or just water. The rats who received the elixirs,as noted by Frances Kelsey Oldham, “shriveled up and died.”
It is worth noting how these victims died:
Victims of Elixir Sulfanilamide poisoning–many of them children being treated for sore throats–were ill about 7 to 21 days. All exhibited similar symptoms, characteristic of kidney failure: stoppage of urine, severe abdominal pain, nausea, vomiting, stupor, and convulsions. They suffered intense and unrelenting pain. At the time there was no known antidote or treatment for diethylene glycol poisoning, no dialysis machines or the ability to do renal transplants.
At the end, S.E. Massengill ended up paying over $500,000 (about $8.45 million today) in wrongful death suits. The company’s owner was also fined $26000 (today about $430,00) for mislabeling and misbranding; by technical definition, an elixir contains alcohol. The chemist, Harold Cole Watkins sadly committed suicide.
Most importantly, Congress passed the Federal Food, Drug and Cosmetic Act of 1938, a law that expanded federal regulatory oversight over drugs and mandated drug safety testing before marketing.

Dr Frances Kelsey Oldham started working at the FDA in August of 1960. She was responsible for the approval of new drugs coming to the market. Back then, the approval process was rather routine. The drug maker had to show that a few patients had take the drug without any ill effects. In September of 1960, the application for the approval of a new drug came across her desk. The drug, thalidomide, was being marketed under the name Kevadon by William S Merrell Co of Cincinnati. It was already on the market since 1957 in Europe, Britain, Canada and the Middle East, where it was used to treat nausea in pregnant women as well as a sedative.
Dr Oldham, working with a chemist, Lee Geismar, and a pharmacologist, Oyam Jiro, initially rejected the application for being incomplete. Early in 1961 came case reports about painful neuropathy in patients on Thalidomide in the British Journal of Medicine. She asked Merrell for more information. Merrell in the interim was mounting it’s own counter offensive, labeling Oldham as an obstructive petty bureaucrat and complaining to the higher-ups in the FDA. Dr Oldham however held her ground.
Dr Oldham had during the WWII also worked on new anti-malarial therapies. At that time, she became aware of the ability of certain drugs to cross the placenta into a fetus with negative consequences. With this in mind, she also asked Merrell to furnish her with any data on fetal effects of the drug. After all, it was being administered to pregnant women. This was in May of 1961. In November 1961, reports began to emerge in Germany and the United Kingdom that mothers who had taken thalidomide during pregnancy were now having babies with severe birth defects – phocomelia. The occurrence of this malformation in an individual results in various abnormalities to the face, limbs, ears, nose, vessels and many other underdevelopments. Although operations can be done to fix the abnormality it is difficult due to the lack of nerves, bones, and other related structures. In all about 4000 babies were affected worldwide. Thalidomide samples given to American doctors were traced, but not all were recovered. Seventeen births of babies with phocomelia were reported in the US.
Merrell pulled it’s application in face of all this evidence.
The efforts of Dr Oldham would have gone unnoticed were it not for coverage in the Washington Post of all her efforts to keep thalidomide off the US market. In August 1962, President John F. Kennedy awarded Frances Kelsey the highest honor given to a civilian in the United States, the President’s Award for Distinguished Federal Civilian Service. Also, Congress passed the Kefauver Harris Amendment or “Drug Efficacy Amendment” in 1962 amendment to the Federal Food, Drug & Cosmetic Act. This amendment required drug manufacturers to provide proof of the effectiveness and safety of their drugs before approval. It provided a proof of efficacy requirement that was not there before. It also required them to provide information of side effects when advertising and stopped cheap generic drugs being marketed as expensive drugs under new trade names as new “breakthrough” medications. It effectively gave us the FDA we have today.